
ABSTRACT
Estimations are that in Ghana, 21% of young girls are mothers by the time they are 18 years old. Unplanned pregnancies among young girls occur mainly due to lack of knowledge about sexuality issues and inappropriate use or non-use of contraceptives. The aim of the study was to determine what influences the choice and use of contraceptives by teenagers in Sunyani west district. The study design was exploratory, descriptive and quantitative. Simple random sampling was used to select respondents from the lists of pregnant teenagers and those having a baby or babies provided by professional nurses in specific health care centers selected for the study. Data was collected by means of a structured questionnaire during respondents’ normal routine visit to the designated health care centers.
Partner preference 36.62% (n=26), absence of side effects 22.54%(n=16) and ease of use 12.65%(n=9) influenced the choice of and use of contraceptives by teenage girls in the study area. Slightly less than half the number of respondents used condoms (46.77%, n=29), oral pill 20.97% (n=13), the same proportion of 20.97% (n=13) used emergency contraceptives and 4.48% (n=3) injectables. Main source of contraceptive information were school teachers, 31.16% (n=24), with family members being the least 10.39 %( n=8). Reasons for discontinuing the use of contraceptives, resulting in pregnancy included side effects 35.62% (n=26), partner dislike 32.88% (n=24) and cost of contraceptives 9.5% (n=7). Respondents suggested improvements in contraceptive use to prevent unplanned pregnancies.
Keywords: Contraceptive methods, choice, influence, side effects, teenage pregnancy.
INTRODUCTION AND BACKGROUND INFORMATION
Pregnancies and childbirth among teenagers are historically common in Ghana. At this age all girls are expected to be pursuing their studies or learning a vocation. However due to a complexity of reasons; economic, social, cultural and religious, many girls from 13 to 19 years find themselves starting motherhood unprepared (Ghana Health Service, 2005:138; Ringheim & Gribble, 2010:17). For many young mothers, however, pregnancy and parenthood mean an early conclusion to their education with consequently reduced career opportunities, increased likelihood that they will find themselves socially excluded and living in poverty (Fraser, Copper, Nolte, 2006:72; Oyadele, Wright and Maja, 2013:95).
The Ghana Demographic and Health Survey (GDHS) (2008) emphasize that knowledge of contraceptive methods is very high among women, 93.4% for girls aged 15 to 19 years and 97.9% for all women. Despite the knowledge about contraception, usage figures among girls aged 15 to 19 years are reportedly very low, resulting in unintended pregnancy.
Teenage pregnancies are generally associated with higher rates of maternal morbidity and mortality and greater risks for clandestine abortions, delivery complications and low birth weight of infants (Ehlers, 2010:15; Oyadele et al., 2013: 97). Furthermore Wekwete (2010:170 mention that teenage girls are vulnerable to sexually transmitted diseases including HIV/AIDS because they are mostly unable to negotiate safe sex. By using contraception effectively, teenage girls would be improving the quality of their own lives and the lives of their children. They will also be reducing the risks associated with pregnancies at such young ages and ensuring that childbirth is commensurate with their family income, autonomy, thereby improving the quality of their own lives and of their children (Durojaye, 2011:1-29; Zungu & Manyisa, 2009). Yeatman and Trinitapoli (2008:1854) argue that, despite a wealth of research describing prevalence of and patterns in the use of modern contraceptive methods in high fertility settings such as sub Saharan Africa, the role of a host of socio cultural factors in facilitating or impeding the effective use of contraception remains only partially understood.
STATEMENT OF THE RESEARCH PROBLEM
Globally, unintended and unplanned pregnancies are highest in Africa. In Ghana, nearly 60% of teenage girls report that their recent birth was unintended (Ringheim & Gribble 2010:19). This occurs because they are not fully matured psychologically, are less prepared and not economically independent. In most cases teenage girls bear the consequence of unplanned pregnancy.
Blanc, Tsui, Croft and Trevitt (2009:68) note that teenage contraceptive use is characterized by shorter periods of consistent use with more contraceptive failure and more stopping for other reasons. Lack of contraception or contraceptive failure by sexually active teenagers pose serious threats to individuals, families and communities. Individual lives and families can be damaged as girls experience frequent, difficult and complicated pregnancies. Teenage motherhood has several disadvantages both to mother and the child and if left unattended, the children to teenage mothers would themselves become teenage mothers thus perpetuating a vicious cycle (Ghana Health Service National Adolescent Health and Development Programme, 2005:138). Though the knowledge of the availability of contraceptives seems high in Ghana, there is a wide gap between knowledge and practice which must be explored.
PURPOSE OF THE STUDY
The aim of the study was to determine the influence on choice and use of contraception by teenage girls in Sunyani west.
OBJECTIVES OF THE STUDY
The objectives of the study were to:
- Determine what influences the choice and use of contraception among teenage girls.
- Describe which contraceptives were most prevalent among teenage girls.
- Identify the reasons for discontinuing contraceptive use.
RESEARCH DESIGN AND METHODS
Research design
The research design was exploratory, descriptive and quantitative. Polit and Beck (2008:20-21) explain that exploratory studies are useful if the researcher wishes to assess and understand a phenomenon in a new light, ask questions and search for new insights, as was the case in this study. Descriptive study designs aim at gaining more information about characteristics within a particular field of study (Burns & Grove, 2005:232).
Research setting
The study was conducted at two health care centers; a public and private health centers in the Sunyani West district, Odomase township, Ghana. The population of the country recorded 24,658,823 with a significant proportion of 38.3% below the age of 15 (Ghana Statistical service, 2013). Health care is the responsibility of the Ghana Health Service (GHS) which is one of the four bodies under the Ministry of Health. Each region has a regional referral hospital under the regional health directorate. There are three independent teaching hospitals which offer specialized services on referrals only.
Population and sampling
The target population comprised pregnant teenage girls in Sunyani west district including those who had a baby or babies at the two selected health care centers for the study. Simple random sampling was used to select respondents from the lists provided by professional nurses at the specific health care centers. Selection criteria included teenage girls between the ages 13 to 19 years; should be pregnant or having a baby (babies); living in Sunyani West district and attending antenatal or postnatal care at the selected health care centers.
Data collection
Teenage girls meeting the selection criteria for the study were invited to participate during their visit to the specific health care centers in Sunyani west district until the required number of 80 (40 respondents from each health care center) was reached. Data was collected by means of a structured questionnaire designed and approved for this research. Each section addressed a specific area that was deemed necessary to understanding the choice and use of contraception among teenage girls. Data was collected during respondents’ normal routine visit to the designated health care centers.
Data analysis
A Statistical Programme for Social Sciences (SPSS) version 16 was used for analysing data. Descriptive statistics such as frequency distribution, and measures of central tendency allowed the data to be organized in ways that gave meaning. Inferential statistics were used in making judgments about the population based on the evidence from the study sample (Burns & Grove, 2005:452).
Validity and reliability
Validity includes truth, strength and value of any findings or conclusions drawn from the data (Grove, Burns & Gray 2013:393). Face and content validity were deemed more applicable for this paper.
Reliability was achieved by conducting a pilot study which produced the same results when repeated for the main research.
ETHICAL CONSIDERATIONS
Permission to conduct the research was obtained from the Research Ethics committee of Health Studies, UNISA and authorities of two health care centers in the Sunyani West district. Ethical standards adhered to throughout the research included; protecting the human rights of respondents, balancing benefits and risks in the study, obtaining informed consent and submitting a research proposal for institutional review (Burns & Grove, 2005:176).
RESULTS AND DISCUSSION
Demographic profile
Respondents’ ages ranged from 19 years, 37.5% (n=30) to 13 years, 2.58% (n=2). Almost 82.28% (n=65) were not married, 16.46 %( n=13) lived with their partners and only 1.27 %( n=1) respondent was married. A total number of 40.63% (n=26) respondents had relatively low monthly income and most respondents, 83.33 % (n=65) were Christians and Muslims, 16.67% (n=13). In this regard, Jones and Dreweke (2011) mention that women of all religious denominations, including Catholics, use contraceptives despite the church’s formal opposition to contraceptive methods other than natural family planning. The conclusion can therefore be made that one’s religious affiliation had no impediment to their use of contraceptive.
Contraceptive knowledge
Most respondents, 82.52% (n=65) had knowledge about contraceptives whilst 19.48% (n=12) lacked contraceptive information. This result tallies with Ghana Demographic and Health Survey (GDHS) (2008), stating that knowledge of contraceptive methods is very high among girls, 93.4% for girls aged 15 to 19 years and 97.9% for all women.
Source of information about contraception
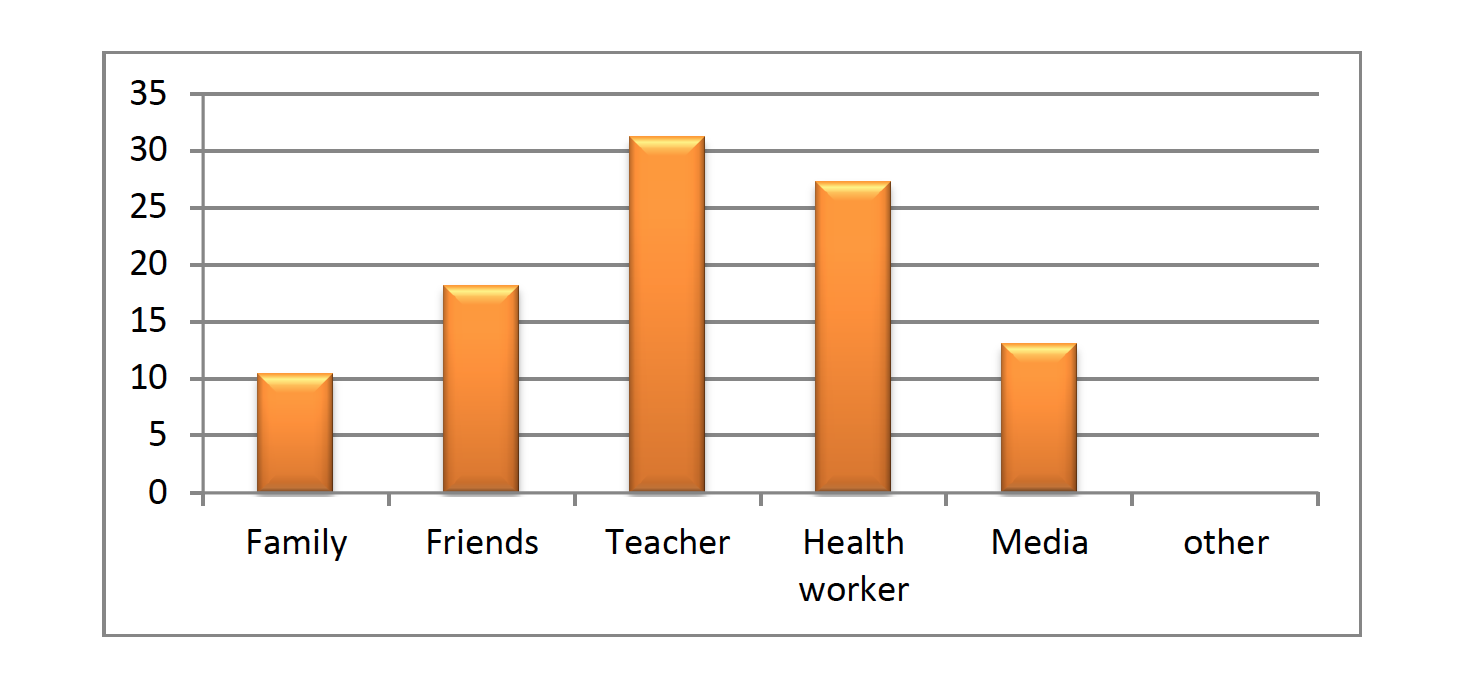
School teachers ranked high, 31.16% (n=24) as the main source of information about contraception, then health workers, 27.27% (n=21) and friends represented 18.18% (n=14). A further 10.39 %( n=8) respondents, were informed about contraception by their family members whilst 12.99% (n=10) got information from the media. In contrast, De Freitas (2007:122) found that the main source of information about contraceptives for adolescents attending the Asa Branca health center in Luanda, Angola was the nurse (28%). Radio and television had 19% and 17% respectively whilst the school contributed 11%. Hagan (2012:125) in a study of 244 students with knowledge of contraception in selected senior high schools in Central Region of Ghana found that 60% of respondents obtained knowledge about contraception from the media (television/radio) and 30% were informed by peers.
Figure 1: Source of information about contraception
Preferred contraceptive methods
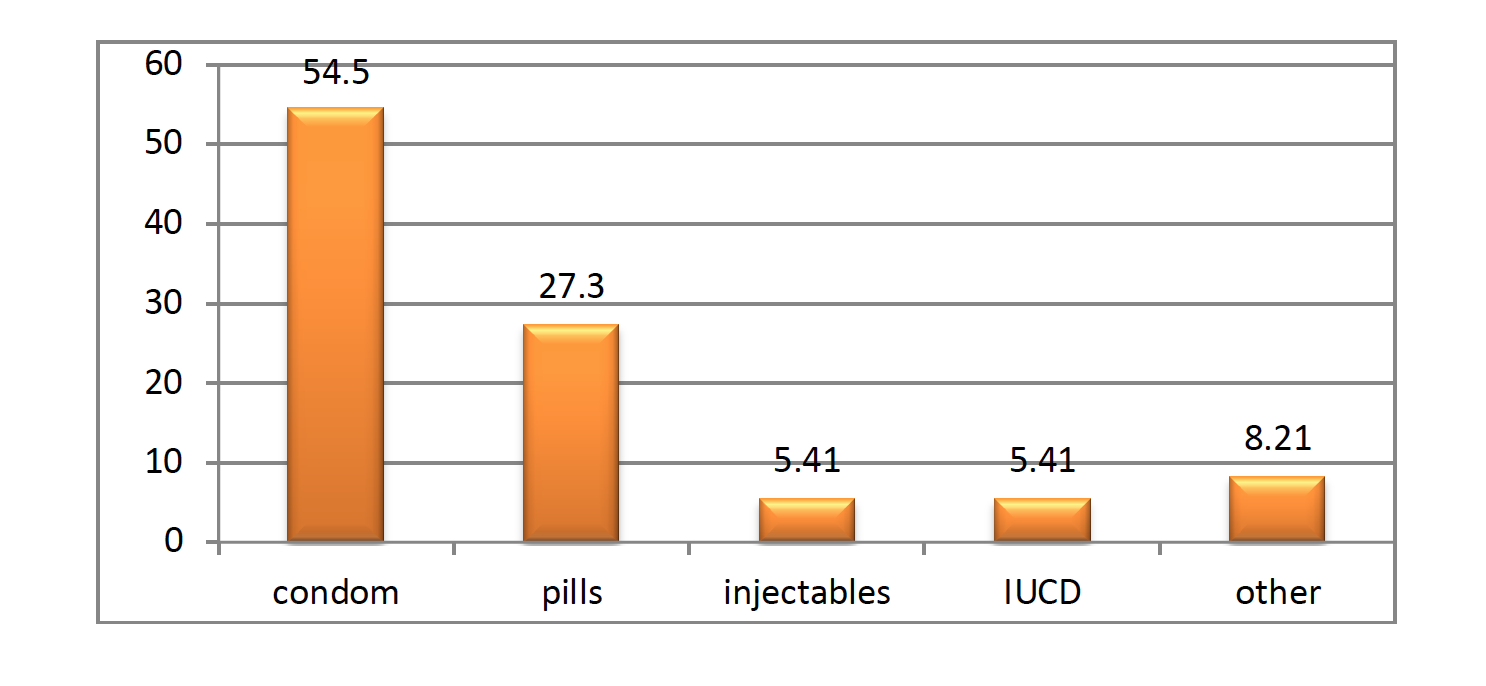
Regarding contraceptive preferences, slightly less than half the number of respondents stated they often used condom (46.77%, n=29), 20.97% (n=13) used oral pill, the same proportion of 20.97% (n=13) used emergency contraceptives and 4.48% (n=3) reportedly used injectables to prevent pregnancy. De Freitas (2007:117) and Hagan (2012:125) found that male condoms were the predominant method used by respondents in similar studies involving adolescents.
Figure 2: Preferred contraceptives used by respondents
Influence on choice of contraceptive method
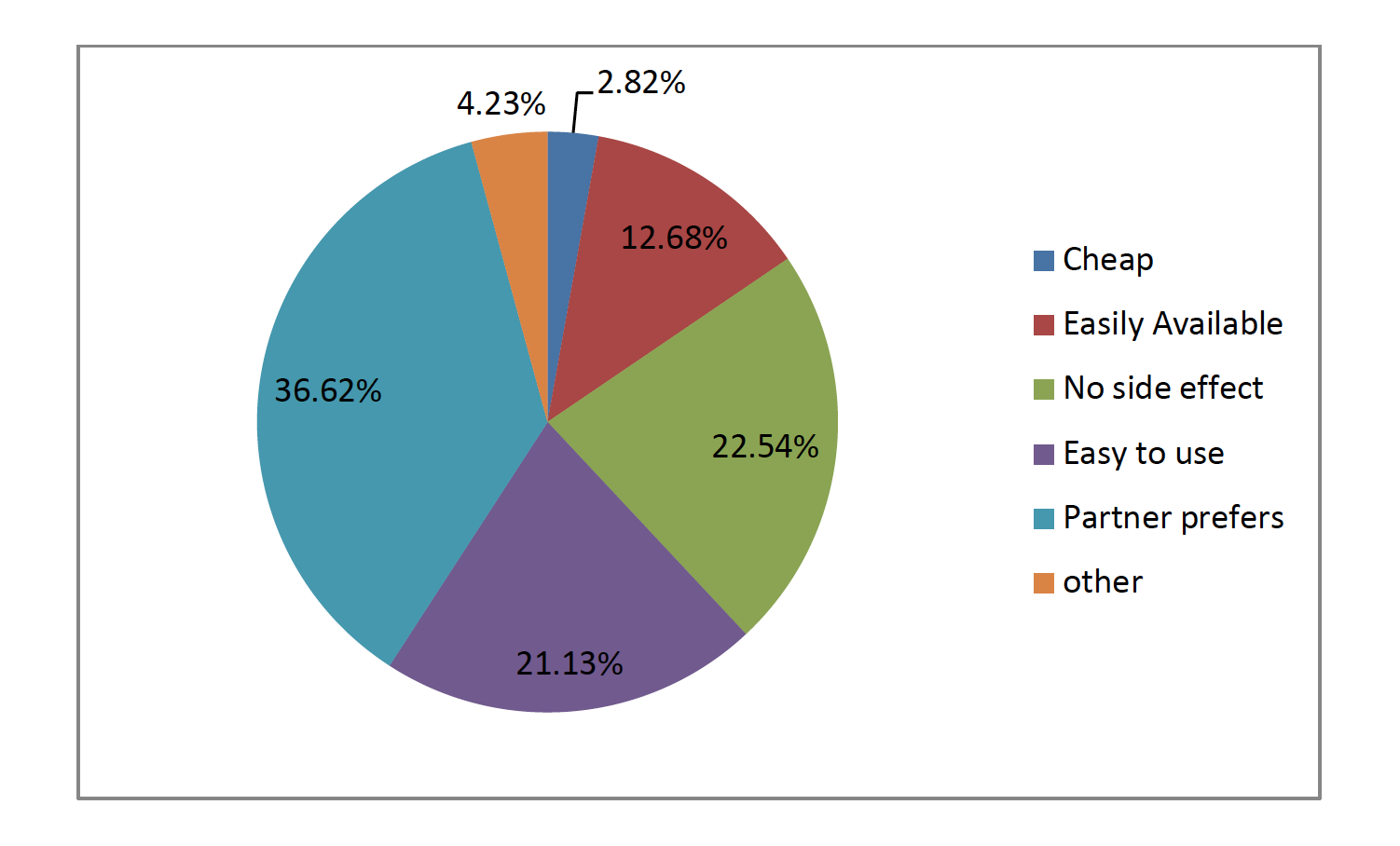
Partner influence was reported as significant in the choice of contraception by respondents, 36.62 % (n=26) and 22.54% (n=16) indicated that it was because the chosen contraceptive had no side effects. Furthermore, 21.13% (n=15) decided to use a specific method because it was easy to use, 12.68 % (n=9) easily available and 2.82% (n=2) felt it was affordable. In contrast, De Freitas (2007:143) report that 43% of adolescent respondents in her study claimed they themselves decided on using contraceptives whilst partners, 26% decided on contraceptives, 21% were influenced by their family and 5% by community or religious leaders.
Figure 3: Influence on choice of contraceptive method
Reasons for discontinuing contraceptive use
Of the respondents, 35.62% (n=26) had stopped using contraceptives due to side effects, 32.88% (n=24) partner dislike of the contraceptive method and the cost compelled 9.59% (n=7) to stop and the same percentage discontinued use due to unavailability. Similarly, Osaikhuwuomwan and Osemwenkha (2013:58-62) found that 68.7% of respondents felt embarrassed or ashamed to use or purchase condom/contraceptives and 50.3% noted it was because male partners disliked condoms.
Side effects of using contraceptives
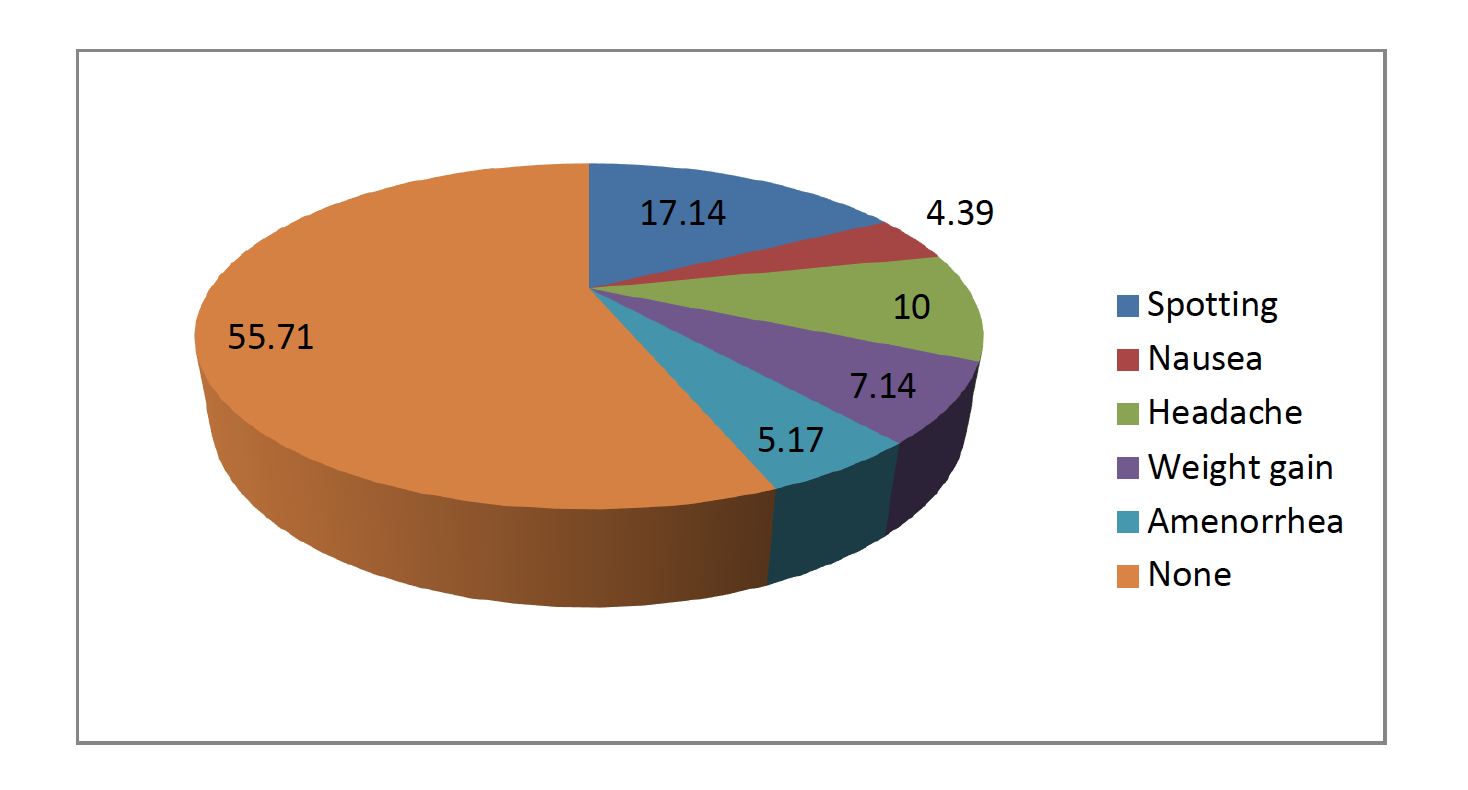
As many as 55.71% (n= 39) had experienced no side effect whilst 17.14% reported to have spotting after the use of these contraceptives, 10% (n=7) experienced headaches, 7.14 % (n=5) had gained weight, (4.39%, n=3) felt nauseas and 5.17% (n=4) had amenorrhea. In their paper titled “Intrauterine Contraception in Adolescents and Young Women: A descriptive study of use, side effects and compliance”, Lara-Torre, Spotswood, Correia and Weiss (2011:39-41) state that 9% of respondents complained of pelvic inflammation disease, 28% of pain, 9% that partner felt strings and 32% complained of bleeding. In contrast, most respondents from this study experienced no side effects. This could be attributed to the fact that the respondents in this study mostly used condoms whereas Lara-Torre et al (2011: 39) specifically examined respondents using IUDs.
Figure 4: Side effects of using contraceptives
RECOMMENDATIONS
Based on the results of the study, the following recommendations are made:
- Focused contraceptive messages on male counterparts
The district health directorate should target young male counterparts of teenage girls with information, education and communication highlighting the advantages of contraceptives used by females like the female condom, the combined oral contraceptive pill and injectables.
- Closer collaboration between district education and health services
Collaboration between the two agencies would increase the capacity of teachers not just to inform the students about sex and contraceptives but to encourage utitlization of contraceptives, inform on side effects of all the choices and encourage abstinence or safe sex among the teenage girls.
- Improved delivery of adolescent health and reproductive services
Adolescent health and reproductive services must be resourced to reach out to more young people; training peer educators, making available contraceptive commodities and providing friendly, stigma free services for the uptake of these services by teenage girls.
LIMITATIONS OF THE STUDY
Generalization of the study’s results might be limited since the study was done in one district- Sunyani West district due to the small sample size. Since contraception involves sexual behavior, some respondents might have felt embarrassed to answer sensitive questions.
CONCLUSION
Results revealed that influences on choice of contraceptives played significant roles in usage of contraceptives by teenage girls in the study area. The choice of contraceptive method used was influenced mostly by the male partners’ preference whilst the decision to stop using contraceptive was influenced by the side effect experienced by the female and the dislike of contraceptive method by the male partner. Condoms were preferred and used by most respondents, followed by oral pill, emergency contraceptives and injectables to prevent pregnancy.
ACKNOWLEDGEMENTS
To all the young women who participated in this study, thank you.
BIBLIOGRAPHY
Burns, N & Grove, SK. ( 2005). The practice of nursing research: conduct, critique & utilization; 5th edition. St Louis, Missouri: Elsevier Saunders.
Burns, N, Grove SK, & Gray, JR. (2014). Understanding Nursing Research: Building an Evidence-Based Practice. St Louis, USA. Elsevier Health Sciences.
De Freitas, E.G. (2007). Adolescents’ knowledge of contraception in a selected area in Angola. Pretoria: University of South Africa
Durojaye, E. (2011). Access to contraception for adolescents in Africa: a human rights challenge in Comparative and International Law Journal of Southern Africa, 44 (1):1-29.
Ehlers, VJ. (2010). Adolescent mothers’ non-utilisation of contraceptives in Zimbabwe. Africa Journal of Nursing and Midwifery, 12(2):14-26.
Fraser, DM, Copper, MA & Nolte, AGW. (eds). (2006). Myles textbook for midwives. London: Churchill Livingstone
Ghana Health Service adolescent health and development programme. (2005) . Training manual for healthcare providers in Ghana. Accra: Government printer.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF Macro. (2009). Ghana Demographic and Health Survey 2008. Accra, Ghana & Calverton, MD, USA. ICF Macro.
Ghana Statistical Service. 2013. The 2010 Population and Housing census report. Accra: Government printer.
Grove, SK, Burns, N & Gray, JR. 2013. The practice of nursing research: appraisal, synthesis and generation of evidence. 7th ed. Philadelphia: Saunders.
Hagan, J. E. (2012) Contraceptive Knowledge, Perceptions and Use among Adolescents in Selected Senior High Schools in the Central Region of Ghana. Journal of Sociological Research, 3(2).
Jones RK, Dreweke J. (2011). Countering conventional wisdom: New evidence on religion and contraceptive use. Alan Guttmacher Institute.
Lara-Torre E, Spotswood L, Correia N & Weiss PM. (2011). Intrauterine Contraception in Adolescents and Young Women: A Descriptive Study of Use, Side Effects and Compliance. Journal of Pediatric and Adolescent Gynecology, 24(1):39-41.
Osaikhuwuomwan JA, Osemwenkha AP. (2013). Adolescents’ perspective regarding adolescent pregnancy, sexuality and contraception. Asian Pacific Journal of Reproduction, 2(1)58-62.
Oyedele, OA, Wright, SCD & Maja, TMM. (2013). Prevention of teenage pregnancies in Soshanguve, South Africa using Johnson Behavioural System Model. Africa Journal of Nursing and Midwifery, 15(1):95-108.
Polit, DF & Beck, CT. (2008). Nursing research: generating and assessing evidence for nursing practice, 8th ed. Philadelphia, USA: Lippincott Williams & Wilkins.
Ringheim, K & Gribble, J. (2010). Improving the reproductive health of Sub-Saharan Africa’s youth, route to achieve the millennium development goal. Population Reference Bureau, Washington DC: Government printer.
Wekwete NN. (2010). Adolescent pregnancy challenges in the era of HIV/AIDS: A case study of a selected rural area in Zimbabwe. Addis Ababa. Organization for Social Science research in Eastern and Southern Africa.
Yeatman, S & Trinitapoli J. (2008). Religion and family planning in rural Malawi in Demographic Research Journal, 19 (55):1854.
Zungu, LL & Manyisa, ZM. (2009). Factors contributing to pregnancies among student nurses at a nursing college in Mpumalanga Province, South Africa. Africa Journal of Nursing and Midwifery, 11(2): 59-74.